By: Carley Langley, BS, EMT-B, SSC & Rich Lindfors, NRP
When it comes to the realm of EMS, not everything is what it seems. If it looks like a duck, swims like a duck, and quacks like a duck, then it must be a duck…right? Theoretically, the quickest and simplest explanation is that yes, surely it is a duck. But what if you came across something that looked like a duck, swam like a duck, and quacked like a duck─ but it turned out to be a horse. As any well-seasoned medic could tell you, it is rare in the field of EMS for things to have an easy explanation, and this edition of the Richmond Condition aims to utilize a recent case study to emphasize that the early detection and diagnosis of sepsis is no exception.

|
But first, what is a “case study”? According to an article published in Evidence-Based Nursing, a case study is “an intensive, systematic investigation of a single individual, group, community or some other unit in which the researcher examines in-depth data relating to several variables” (Heale & Twycross, 2018). It is an excellent way to disseminate important information about a broad topic. However, it differs from other types of scholarly research because it is more relaxed and less-data driven, taking more of a casually-educational tone and style. This particular case study will review a call taken by the Richmond Ambulance Authority in Richmond, Virginia in early 2019.
A Curious Case of Sepsis
Imagine yourself as a paramedic in the city of Richmond during the winter of 2019: the morning weather has all the indications that it is going to be a great day on duty. The air is crisp and cold; the sun is out with scarcely a cloud in the sky.
You and your partner are debriefing about the night’s calls when you hear the emergency tones sound through the tablet. You instinctively sit up to attention as a familiar voice comes over the radio, “M89, start priority one, reference a fall.” As your partner begins emergently navigating the early morning traffic, updated information comes through regarding the patient following the communication center’s interrogation: the patient had not fallen, but instead merely needed assistance getting from his house to his car. As a result, the call gets “downgraded” to a non-emergent response (because there were no immediate life threats) and you relax in your seat in preparation for a simple public assist.
When you arrive on the scene, there is a small gathering of people, but no immediately obvious hazards or life threats. A firefighter waves you into the fray, greeting you with a brief update on the situation. The family explains the patient lives alone and has been increasingly ill for the pasts five days with a fever that was being “controlled” with OTC (over-the-counter) Tylenol®. The family had noted a decrease in his overall mental status, a decline in his appetite, and a description of symptoms consistent with dehydration. Family on scene also note to you the patient’s home felt “quite cold” when they entered today and found it odd, as the patient usually kept the house very warm.

|
The primary impression as you approach the patient is poor. His eyes only open as you introduce yourself and begin the assessment, and then slowly close back. You reach out to feel for and find a radial pulse, but there is none palpable. His skin feels cool to the touch, and his breathing is shallow and infrequent. His family on scene states he only knows his name and where he is, but that he is typically more awake and alert at baseline. He seems generally confused, and only appears to withdrawal his limbs from painful stimuli. Attaching the patient to a cardiac monitor reveals a heart rate in the upper forties with 4-lead ECG confirming the bradycardia. The patient is found to be hypotensive with a systolic blood pressure of 90. Every sign and symptom directs you to the conclusion that the patient is suffering from a textbook case of environmental hypothermia. All doubts are erased from your mind when you obtain temperature, and the tympanic thermometer only reads “LOW.”
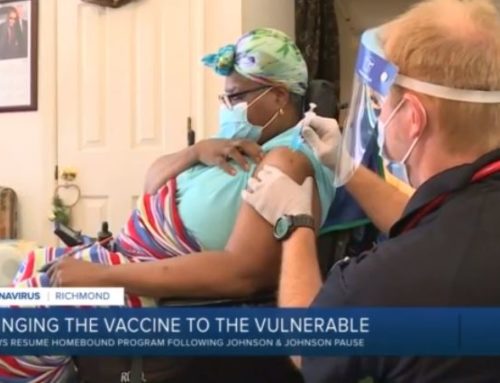
How do you decide to treat the patient? The paramedic who ran this call, [name withheld], began treating the above patient for a case of sepsis with possible environmental hypothermia. Intravenous (IV) access successfully obtained, and fluids administered immediately. Two 0.5 mg doses of atropine were pushed via IV 10 minutes apart during transport. Cardiac monitor defibrillation/pacing pads placed on the chest as a precaution and the patient was transported emergently to the nearest hospital.
You notified the facility of your impending arrival, and as you push the patient and stretcher into the hospital a nurse guides you into a nearby hospital room. During the report at the bedside, she prepares the re-warming supplies at the bedside and adjusts the temperature on the thermostat. You finish your turnover of the patient and share your on-scene findings including the possibility of sepsis. However, as you walk out of the room the bed light overhead flashes red and the ED intercom keys up. “Code sepsis!” the notice declares the room number for the patient you just delivered nursing staff rush in to assist.
Sepsis: More than just a Fever
The hospital certainly believed the patient was critically ill and agreed with your diagnosis. As the reader it has probably been made abundantly clear to you that the patient, despite his classic presentation for environmental hypothermia, was actually in the late stages of a septic infection. The hospital was able to stabilize and replete the patient, and his septic infection tempered with vigorous antibiotics over several days. A week later, the patient was discharged from the hospital and back at his baseline. However, the outcome could have been much more severe if the medics had failed to recognize the (albeit, subtle) indications of advanced septic infection. So, what can we learn from this case study
Sepsis Basics
The point of the above case study is to emphasize the vast array of ways that a septic infection can present as and highlight the importance of recognizing these various presentations early on for more successful patient outcomes — equipping all current EMS personnel with a strong understanding of the various stages of sepsis and how to recognize them in the earliest stages.
But what even is sepsis? Even in a country at the forefront of advanced medical practices, sepsis remains one of the top causes of death in the United States and is the number one reason for death amongst non-coronary ICU patients across all U.S. hospitals (Mayr, Yende, & Angus, 2014). But despite its prevalence throughout the healthcare field, an exact definition of what constitutes “sepsis” has been difficult to identify, as its criteria for a long time varied widely by region, facility, and practitioner as well as whether the definition is within an administrative, scientific, or clinical context.
Colloquially speaking, the terms “sepsis,” and “septicemia,” and “bacteremia” (also occasionally erroneously referred to as “blood poisoning,” despite it having nothing to do with poison) are often used by EMS personnel to describe any wide-spread inflammatory response. While not completely incorrect, according to the U.S. CDC’s definition, sepsis is “the body’s extreme reaction to an infection” of any origin (Center for Disease Control and Prevention, 2018). When a patient “dies of sepsis” what it means is that a small source of infection or inflammation became so advanced and widespread within the patient’s body that ultimately the circulation of blood was compromised. As the patient’s tissues began to receive less blood flow, the patient’s organ systems began to dysfunction and eventually failed (signs and symptoms are not limited to one body system).
However, in 1991 the American College of Chest Physicians and the Society of Critical Care Medicine Consensus Conference collaborated to combat this confusion and construct an organized framework that more strictly categorized the progressively worsening stages of sepsis starting with SIRS (Systemic Inflammatory Response Syndrome), sepsis, and then severe sepsis, defining specific criteria required for meeting each stage that is still referenced today (Mayr, Yende, & Angus, 2014). If any initial infection becomes septic and is left untreated, patients can go into septic shock, a highly dangerous type of shock that can easily become fatal.
Who is at risk for sepsis, and how do you get it?
In truth, anyone who has an infection (e.g. fungal, bacterial, viral) is at some risk for developing a septic infection until fully recovered. However, there are some patient populations who are a much higher risk for developing it, including elderly people (aged 65+); children younger than one year of age; pregnant women; people who are immunocompromised; and people with chronic medical conditions such as heart failure, diabetes, or cirrhosis (Mayo Clinic Staff, 2018). When compared with the rest of the general population, males and people of African-American descent are also at an increased risk for developing sepsis at some point throughout their lifetime (Center for Disease Control and Prevention, 2018). Also, people with open wounds/injuries or who have recently undergone surgery are also at a heightened risk for developing an infection that could easily progress to sepsis.
Sepsis can also originate from within any part of the body or from any tissue inflammation (e.g., pneumonia, influenza, urinary tract infection, open leg wound) and progressively spread. Statistically speaking, the most common sources of sepsis are infections of the respiratory, urinary, and digestive tracts (Mayo Clinic Staff, 2018).
In terms of causative agents, any infection can progress to sepsis, but gram-negative organisms are responsible for almost twice the frequency of infection incidence than their gram-positive counterparts (GS Martin, 2003). Among the huge array of bacterial organisms, the most proliferate instigators are Staphylococcus aureus (20.5% of cases studied), Pseudomonas species, Enterobacteriaceae (mainly E. coli), and fungi (19%).
How can the stages of sepsis be recognized?
Most people recover from mild sepsis, whereas the mortality rate among patients with septic shock is 50% (Mayr, Yende, & Angus, 2014).
It is of importance to note that as current physician’s understanding in regards to the epidemiology of sepsis continues to grow, the definition and guidelines for identifying and treating SIRS, sepsis, and septic shock will most likely continue to evolve as well. All EMS personnel, regardless of rank or experience are encouraged to remain inquisitive and up-to-date on all sepsis-related literature to maximize positive patient outcomes.
How is sepsis treated in the pre-hospital environment?
Septic patients require plenty of IV fluids to replenish their circulatory system and replete against dehydration, as well as an immediate initiation of a regimen of broad-spectrum antibiotics (if the source of infection is unknown) begun in a hospital setting under close medical supervision (Mayo Clinic Staff, 2018). After cultures are identified, more specifically-target antibiotics may be administered.
In the pre-hospital environment, the treatment plan begins with us. The importance of knowing the early signs and understanding the severity of the late signs of this deadly disease can be the difference between life and death. The case described herein could be confusing due to the confounding circumstances (outside cold temps, cold patient, etc.). Because of this medic’s thorough understanding of sepsis, the patient received IV fluid resuscitation and atropine to combat the sepsis.
How should you document this case?
As with any call, you must carefully consider the details and circumstances before writing your electronic Patient Care Report (ePCR). This call leads the reader to a conclusion of a textbook case of environmental hypothermia. Or did it? As the Quality Assurance (QA) officer each case presents questions, and the top three questions include:
- Were my conclusion(s) based solely on the ePCR or did circumstantial evidence plays a role (i.e. the weather, time of year, season)?
- Was the care provided to the patient consistent with a standing protocol or with any other standard of practice?
- If the same type of case were presented to me, would I have done anything differently?
Presented with this case, I had immediate concerns about the care provided to the patient. Why would a case of environmental hypothermia have this medication administration? Why would a seasoned paramedic give atropine to a patient not having a cardiac or another type of event where this drug would be indicated? This care is not consistent with any standard known to me or any protocol in our organization or region. Met with the same circumstances, I would have performed differently. In reality a host of other questions flooded me when I read this case. Rarely is there a time when disciplining a medic crosses my mind, but, this case may change all that. I reached out to the medic and what I thought was going to be a learning opportunity for them was, in reality, education for me and the reason for this article.
On the first read of the report, I thought, as many of you did, this patient was only suffering from environmental hypothermia or at the least was the prevailing condition at the time. However, after discussing the case with the crew who responded, they explained how this duck on paper became a horse. Documenting a complex case such as this can be one of the most challenging skills we face.
Documentation
This case study developed because of documentation. As EMS providers, there is a direct correlation between the care we provide, the documentation we provide and the outcome for the patient. The documentation provided by this medic hurt the evaluation of this case. If required, would this medic be able to prove the care they provided was consistent with standard medical practice? My answer would most certainly be, no.
References
Center for Disease Control and Prevention. (2018, June 22). What is Sepsis? Retrieved from Center for Disease Control and Prevention: https://www.cdc.gov/sepsis/what-is-sepsis.html
Duck2.jpeg. (2008, May 21). https://commons.wikimedia.org/wiki/File:Mallard2.jpg. Wikimedia Commons.
GS, Martin, D. M. (2003). The Epidemiology of Sepsis in the United States. New England Journal of Medicine.
Heale, R., & Twycross, A. (2018, January). What is a case study? Evidence-Based Nursing, 21, 7-8. doi:10.1136/eb-2017-102845
Johns Hopkins Medicine. (n.d.). What is Septicemia? Retrieved from Johns Hopkins Medicine: https://www.hopkinsmedicine.org/health/conditions-and-diseases/septicemia
Mayo Clinic Staff. (2018, November 16). Diseases and Conditions: Sepsis. Retrieved from Mayo Clinic: https://www.mayoclinic.org/diseases-conditions/sepsis/symptoms-causes/syc-20351214
Mayr, F. B., Yende, S., & Angus, D. C. (2014, January 1). Epidemiology of severe sepsis. Virulence, 5(1), 4-11. doi:10.4161/viru.27372
SEEDREAM, Shutterstock. (n.d.). Sick Old Man Sitting On the Sofa with a Cold. https://www.shutterstock.com/video/clip-9339362-sick-old-man-sitting-on-sofa-cold. Shutterstock.